The essay below isn’t our usual essay on leadership, but we hope you’ll take about seven minutes to read it and benefit from it. We believe there are a couple of opportunities worth harvesting from the COVID-19 challenge.
First, history will judge organizational leaders by how they lead in these difficult times. We all now have especially good reason to be and show our best. It’s also a chance to step back and ask ourselves how we can use this challenge to create even more agile and resilient organizations. Do we have processes that could be improved so our organizations are not overly dependent on a few, critical few superheroes? Is everyone clear about their priorities – the organizational OUTCOMES that matter most? Are communications about COVID-19 or ANY other critical issues being handled effectively and at every level of leadership? Are there new ways of doing things that could help minimize the temporary inconveniences imposed by this current challenge? Maybe it’s an opportunity to hear what employees have to say, and to pilot some fresh ideas. And so on.
Second, and more broadly, there are some interesting lessons to be learned from previous big challenges, like the 1918 flu pandemic. We don’t know yet whether or not COVID-19 will become such a crisis, but sometimes history, and the lessons learned, can inform actions that prevent or dampen crises.
With that in mind, the following essay was originally intended just for ELG associates by an ELG associate. It’s a solid review and comparison of the 1918 flu and what we know so far about COVID-19. Our team found it useful. Yours might, too.
Wendi Peck & Bill Casey
11 March 2020
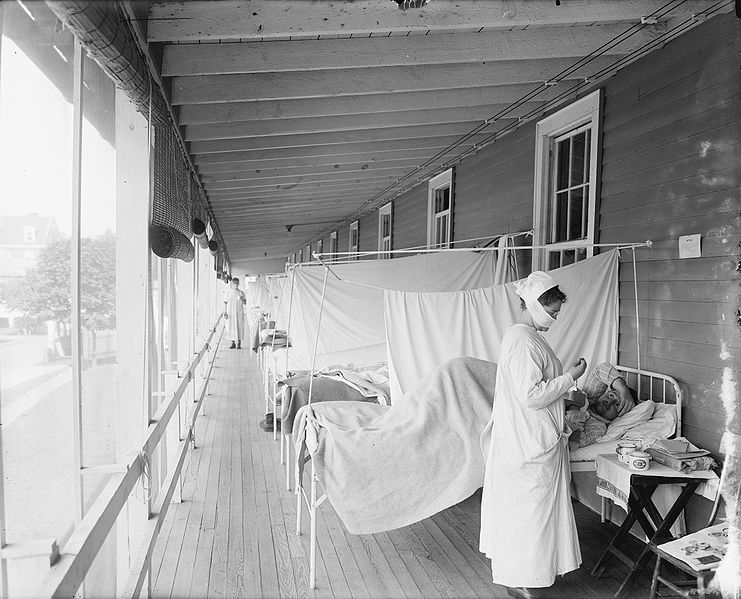
Lessons from the 1918 Flu Pandemic
Cassandra Letkomiller RN, BSN
As a medical professional and amateur historian, I’ve long been fascinated by the 1918 flu pandemic, and have presented on the topic a few times to historical societies. That pandemic was a major, world-changing event. Yet, most well-educated adults haven’t learned much about it, nor did they need to. But now, because of the recent COVID-19 outbreak, it may be worth looking for parallels and differences – and lessons. I hope COVID-19 isn’t another such world-changer. Maybe the lessons of history will help us prevent that.
Quick Synopsis of the 1918 Flu Pandemic
In 1918 science had made great strides since the discovery and application of germ theory. With the advent of germ theory and knowledge of proper hygiene, lifespan increased dramatically. Before this advent, nearly 50% of all children born died before the age of five years. When you see the young average lifespan numbers before the turn of the century, it is in large part the high proportion of death in babies and young children, which drew down this average dramatically. Armored with germ theory, the idea of germs causing massive loss of life seemed a part of a dark past filled with ignorance. It was the modern age in 1918! The middle class in cities in the USA enjoyed electricity and indoor plumbing with clean water.
However, death was still lurking in the shadows and about to take an unusual form. The 1918 flu began in spring 1918 and was like the typical flu. Since WWI was raging, it quickly moved across the ocean via soldiers in crowded conditions. Europe felt the flu in the summer of 1918, and when it came back to the US in fall 1918, it had become much more lethal. From fall to spring 1918/19, the world was caught by surprise, and in the end (estimates vary), roughly 50–100 million people died worldwide. The virus died down in summer 1919 but still reared its head again in the fall/winter of 1919-20 before vanishing entirely. The virus made its way throughout the entire world, even islands and northern Inuit tribes were decimated. Australia is the only country with such strict quarantine measures from start to finish that it was not affected. Elsewhere, the 1918 flu caused so many deaths that mass graves were dug, morgues overflowed with corpses, the economy and supply chains slowed dramatically, quarantines were placed, and communities were forced to band together to survive.
So far, COVID-19 bears many scientific markers that nearly match 1918 flu, so it is possible to see some similar consequences as a result now, while the virus is not yet well contained.
Similarities & Differences Between COVID-19 (Coronavirus) & 1918 Flu
- Case fatality rate (CFR) – Estimates vary somewhat, but 1918 had a CFR of 2-3% according to Wikipedia and other related sources. Higher estimates are somewhere under 5%. COVID-19 kills around 3.4%, according to the World Health Organization a few days ago. Flu this past year, on the other hand, has had a CFR of 0.05%.
- Remember, too, that back in 1918, we didn’t have the benefit of antibiotics for secondary pneumonia caused by the flu yet, or intubation, or antivirals and steroids to assist the body somewhat. COVID-19 is killing close to the same numbers as 1918 flu with the advantages of most modern medicine in the world.
- “R0”, the measure of how contagious an infectious disease is – R1, for example, denotes an infection rate at which one infected person will, on average, infect one other person. For COVID-19 the R0 is estimated at 2.2, though some epidemiologists who reviewed 12 studies focused on China and overseas estimated a range of 1.4 to 6.49. Quarantine and containment measures have helped slow it down. The 1918 flu had an R0 of 1.47- 2.27.
- Both COVID-19 and 1918 flu attack the lungs and cause a high fever. We are unsure of the incubation period of 1918 influenza, but in both cases, a person would sometimes have a mild to moderate infection, and then recover. (Both viruses are highly aerosolized – i.e., easily transmitted by air). Other people would rapidly go from health to having difficulty breathing and then die in a matter of mere days. Both viruses also produce a higher number of complicated or severe cases that require hospitalization, much of that from secondary bacterial pneumonia.
- COVID-19 attacks a different patient population than 1918 flu by far, but both viruses go after groups in patterns not entirely typical of a usual flu season. In 1918 the flu hit healthy adults aged 20-40 years, especially hard. The robust immune system of young adults seemed to cause a “cytokine storm” or over-reactive immune response, which killed patients. Children, and especially the elderly, caught the 1918 flu less. COVID-19 favors killing the elderly and men more than women.
- 1918 flu was estimated to have infected about 30% of the American population. Dr. Marc Lipsitch of Harvard T.H. Chan School of Public Health believes that as much as 40-70% of the American people could become infected with COVID-19 on some level.
- In 1918 more Americans lived rural lives rather than urban (i.e., 50% rural, 50% urban)...
- In both cases, governments’ responses and record keeping were inconsistent, which presented issues.
- In both cases, the attempt at creating a vaccine occurred.
Conclusion
There once was a king who wished to reward his loyal advisor, telling him, “As reward for your service, you may have anything in the kingdom. Just ask.” The advisor, pointing to a chessboard, said, “My desires are modest, Sire. Please just give me one grain of rice for the first square, two grains for the second square, four for the third square, and so on . . .” The king, no fool, got the joke – 1x263 grains of rice would have bankrupt his kingdom. Such is the nature of exponentiality: it starts modestly, but that’s not where it ends up.
The 1918 flu did not go on forever, but it was exponential for too long, taking too great a toll. Surely, our job today is to stop the exponentiality of COVID-19 before it runs its own course.
Today, we have advantages not available a century ago. Medically, our ability to treat pneumonia is hugely improved.
One exciting development is that scientists are communicating and collaborating globally.
Governments, too, are better poised than a century ago.
Of course, our ability to communicate almost immediately and globally means that telework is a possibility for many of us.
I don’t mean any of my hopeful observations to be mistaken as counsel for laxness or lethargy.

Leave a comment!